

The commercial real estate landscape continues to evolve. In a post-pandemic world, adaptive reuse is a trend to closely follow moving forward. With the national office vacancy rate north of 17%, we’ve seen trends of office space evolution into multifamily, science and technology and other sectors. Medical facility construction is expected to increase in the next few years, driven by the gradual aging of the U.S. population and subsequently, an increased demand for healthcare services.
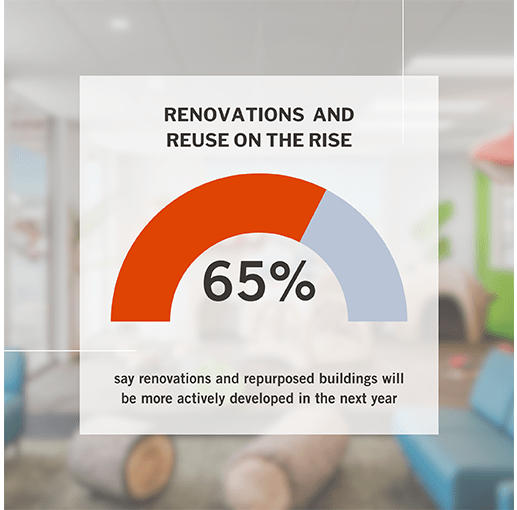
In data collected from Ware Malcomb’s ongoing research efforts, our recent Pulse Survey shows 49% of respondents anticipate a heightened emphasis on office conversion into medical spaces over the next three years. This aligns with the broader sentiment that repurposing existing structures will outpace ground-up construction. Two-thirds of survey participants foresee escalating renovation and adaptive reuse endeavors, particularly targeting office spaces.
The distinctions between general office spaces and healthcare facilities can be stark, making transitions difficult in some cases.
Parking ratios, which average about one space per 250 square feet for office facilities, need to be about one space per 180 square feet for medical office buildings to allow for more parking options. Parking is a major factor in ultimately deciding to move forward with a conversion, but if space is limited, there are some options to consider. These include:
- Adding a parking structure
- Shared parking with adjacent buildings
- Acquiring open land
- Repurposing adjacent property
- Negotiating with the city using their codified process
In addition to having more parking options, the ADA parking stall ratio may be greater than the standard 2% depending on the type of clinic. Larger drop off areas are also needed.
Medical office buildings necessitate unique requirements that set them apart from conventional office buildings. These requirements include features such as:
- Ducted return systems
- Dual levels of air filtration
- Emergency power setups
- Gurney elevators
- Wider exit stairs
- Specialized storage for medical gases and waste
In addition, possible structural adjustments may be needed to accommodate heavy equipment like X-ray machines, lights, and hyperbaric chambers to minimize building vibrations during procedures. Floor to floor heights in areas such as surgery or imaging rooms warrant special attention to ensure equipment can fit inside while allowing for optimal functionality.
We provided interior architecture and design services for Mini Pearl IVF in San Diego, Ca., converting a former bank suite into a 6,000 square foot clinic with an embryology lab, andrology lab, phlebotomy space, procedure room and PACU. This is one of multiple former bank suites our firm has converted.
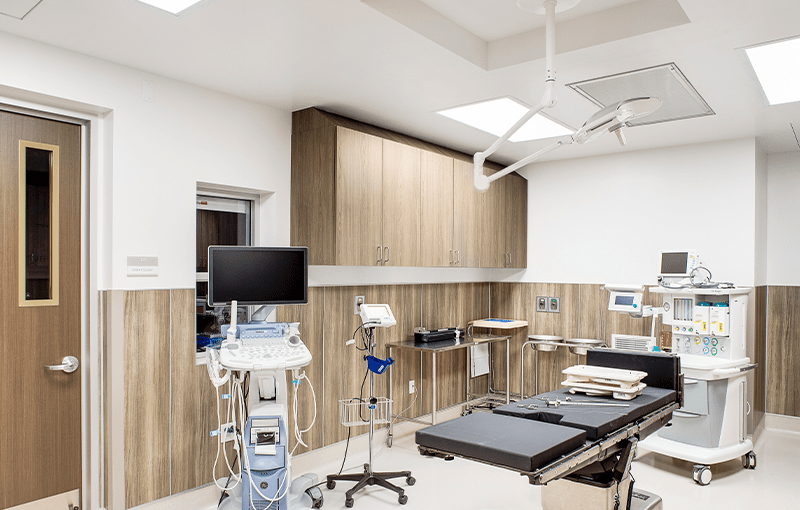
In order to accommodate the necessary equipment for the embryology lab, which included the placement of an air handling unit in the above ceiling plenum, it was required that our team demolish the ceilings out of the suite. The floor to deck height was approximately 12 feet, 6 inches and the ceiling needed to be lowered to approximately 8 feet to accommodate this large piece of equipment.

Enhancements to the MEP (Mechanical, Electrical, and Plumbing) building systems are often necessary in medical office buildings as there are heightened demands for heating, ventilation, air conditioning. HVAC supplies also need to support stringent filtration and ventilation standards. In Mini Pearl IVF, a large amount of electrical equipment was installed, including a 24-hour backup generator.